
When Is It More Than Just Picky Eating?

Many parents reach a point where they wonder: Is this just a phase, or is something more going on? Feeding challenges can look very similar on the surface. One child refuses vegetables, another eats only a handful of foods, and suddenly terms like picky eating, Pediatric Feeding Disorder (PFD), and ARFID start appearing in searches. It’s understandable to feel unsure.
This blog explains the differences between picky eating, Pediatric Feeding Disorder, and ARFID, where these challenges can overlap, and how to recognize when feeding difficulties may be more than a typical developmental phase.
Picky Eating: What Is Usually Part of Normal Development?
Picky eating is extremely common in early childhood and is often a normal part of learning how to eat. As children develop independence, preferences, and opinions, food becomes an easy place for this to show up.
A child who is picky may strongly prefer certain foods, reject foods they once accepted, or hesitate around unfamiliar foods. Even with this selectivity, most children with typical picky eating are still able to eat foods from all major food groups over time, maintain stable growth, and gradually expand their diet.
Food neophobia—hesitation or fear around new foods—is a normal developmental stage. It typically begins around 12 months, intensifies around 18 months, peaks between ages 2 and 6, and gradually fades after age 7 (Dovey et al., 2008). While this phase can feel challenging, it usually improves with repeated exposure and supportive mealtime routines.
What distinguishes picky eating from a feeding disorder is impact. Typical picky eating does not interfere with growth, nutrition, feeding skills, or overall family functioning in a significant or ongoing way.
What Is Pediatric Feeding Disorder (PFD)?
Pediatric Feeding Disorder (PFD) is a medical diagnosis that looks beyond food preferences and considers how feeding challenges affect a child’s health, development, and daily functioning. PFD can be evaluated and diagnosed by qualified healthcare professionals involved in pediatric feeding care, including speech-language pathologists (SLPs), occupational therapists (OTs), and dietitians and other healthcare professionals often within a multidisciplinary team.
PFD is defined as impaired oral intake that is not age-appropriate and is associated with dysfunction in one or more of four areas: medical, nutritional, feeding skill, and psychosocial.
A child does not need to struggle in all four areas to meet criteria—impact in just one domain is enough.
In practice, PFD may involve medical contributors such as reflux, breathing or swallowing difficulties, or gastrointestinal discomfort; nutritional concerns like difficulty meeting needs through diet alone; feeding skill challenges such as chewing or swallowing difficulties; and psychosocial stress that affects the child, the family, or both.
PFD focuses on how a child eats and how feeding functions overall—not just which foods are accepted.
What Is ARFID?
Avoidant/Restrictive Food Intake Disorder (ARFID) is an eating disorder diagnosis defined in the DSM-5-TR. ARFID involves restricted food intake that leads to nutritional, growth, or psychosocial impairment, without any concerns related to body image or weight. Because ARFID is a mental health diagnosis, it must be evaluated and diagnosed by a qualified mental health or medical professional, such as a psychologist, psychiatrist, or physician, often as part of a multidisciplinary team.
Children with ARFID are not avoiding food because of how they want their body to look. Instead, restriction is driven by one or more patterns. Some children show little interest in food or have a consistently low appetite. Others have extreme sensory sensitivities to the taste, texture, smell, or appearance of food. A third pattern involves avoidance due to fear of adverse consequences, such as choking, vomiting, or allergic reactions.
A child may fit one pattern or experience a combination of all three, and these patterns can shift over time. ARFID is often associated with significant anxiety around eating and a very narrow range of accepted foods. Feeding skills may be adequate, but the emotional and psychological response to food interferes with daily life.
Why These Feeding Challenges Can Look Similar
Pediatric Feeding Disorder and ARFID can look very similar from the outside, particularly when a child eats a limited variety of foods or mealtimes feel stressful. This overlap is one reason families often feel unsure about what applies to their child.
The difference lies in what is driving the difficulty. PFD is grounded in medical and developmental factors and often includes feeding skill challenges or medical contributors. ARFID is classified as an eating disorder and is primarily driven by fear, anxiety, or sensory avoidance, even though medical and nutritional support may still be part of care.
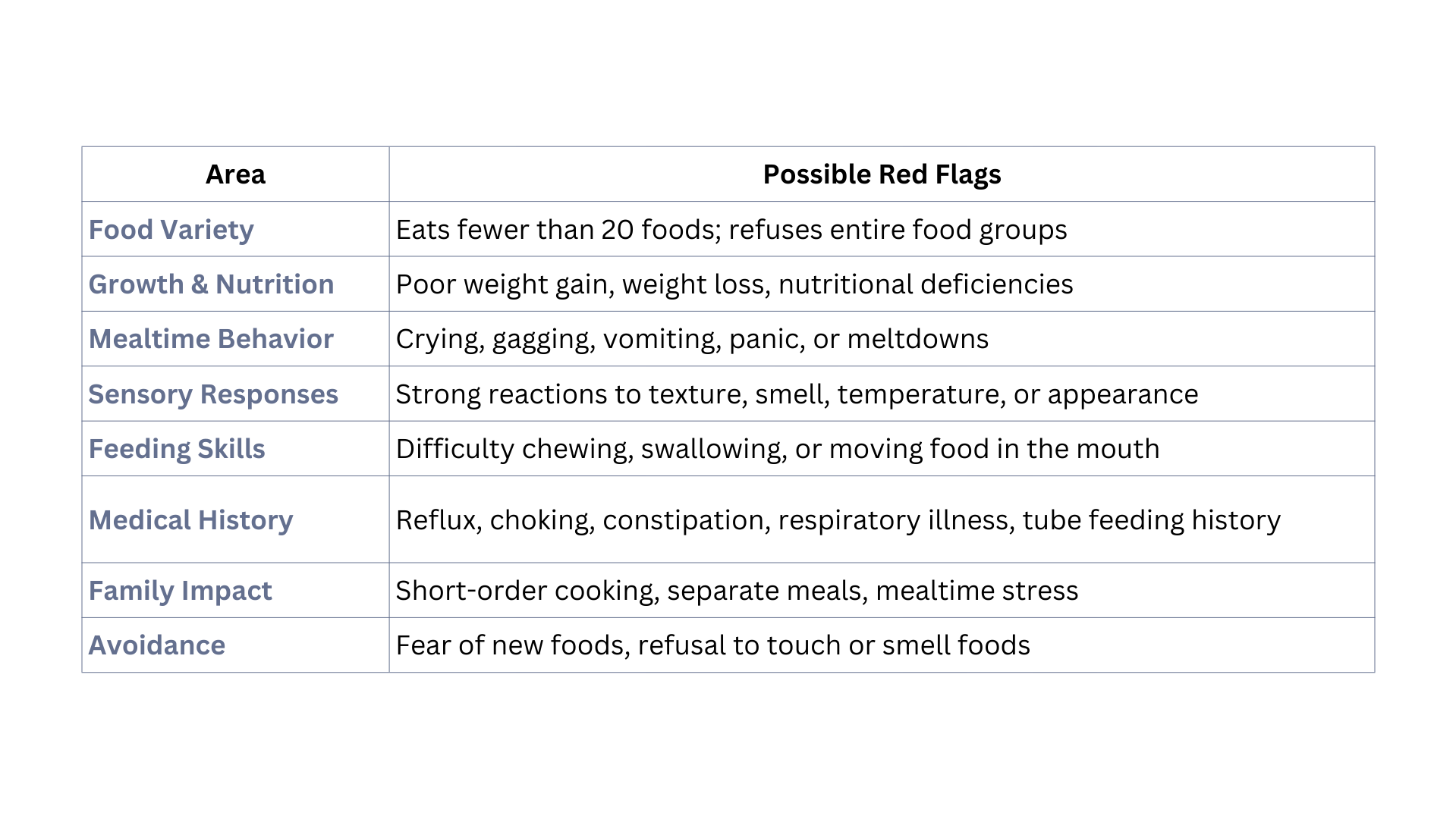
General Signs and Symptoms That May Signal a Feeding Disorder
Rather than fitting neatly into one category, many feeding challenges share common signs. These do not automatically mean a diagnosis is present, but they may indicate that feeding is affecting more than preferences.
How Common Are Pediatric Feeding Disorder and ARFID?
Feeding challenges are far more common than many parents realize. Research suggests that 25–45% of typically developing children experience feeding difficulties at some point, and up to 80% of children with medical conditions or developmental disabilities develop feeding disorders (Davies et al., 2006; Delaney & Arvedson, 2008).
ARFID is relatively uncommon in the general population, with prevalence estimates ranging from approximately 0.3–3% (Micali et al., 2011; Hay et al., 2017). Rates are higher in specialty medical and eating disorder treatment settings, estimated between 5–23% (Norris et al., 2012; Fisher et al., 2014; Nicely et al., 2014; Kurz et al., 2016).
When to Seek Support
If feeding challenges feel ongoing, are affecting your child’s growth, nutrition, feeding skills, or are creating consistent stress around meals, it may be helpful to reach out for guidance.
A feeding consultation offers a space to talk through your concerns, better understand what may be influencing your child’s eating, and identify which areas of feeding may be impacted. For some families, this brings reassurance. For others, it helps clarify next steps—whether that involves support for picky eating, further evaluation for Pediatric Feeding Disorder, or referral to additional providers when appropriate.
If you’re feeling unsure, you don’t have to navigate this alone. Early, thoughtful support can help reduce stress around meals and protect your child’s relationship with food over time.
This article is for educational purposes and does not replace individualized medical or therapeutic care.